Soviet field medicine in Afghanistan
- Elaine Hasty
- Mar 7, 2024
- 4 min read
Updated: Apr 5, 2024
Afghanistan's rugged mountains and it's extremes of climate gave challenges unlike any before to the Soviet field medicine. With it's dry climate, high temperatures in its unbearably hot summers, impure water sources adding to the difficulties to the doctors and nurses tending to the ever increasing sick and wounded Soviet soldiers, the immediate problems to be dealt with was getting the wounded from the battle field to field hospitals.
Speed means life
Timing became a matter, literally, of life and death for each soldier wounded. Helicopters could not necessarily reach the required altitude where the soldiers were meaning those lightly wounded, without evacuation, their wounds quickly became serious. Soldiers with serious injuries died where they lay. With the helicopters unable to reach the wounded at such altitudes meant the task of trying to bring the injured to an altitude the helicopters could land, this took some 13-15 able bodied men to get one wounded man to a pick up point.

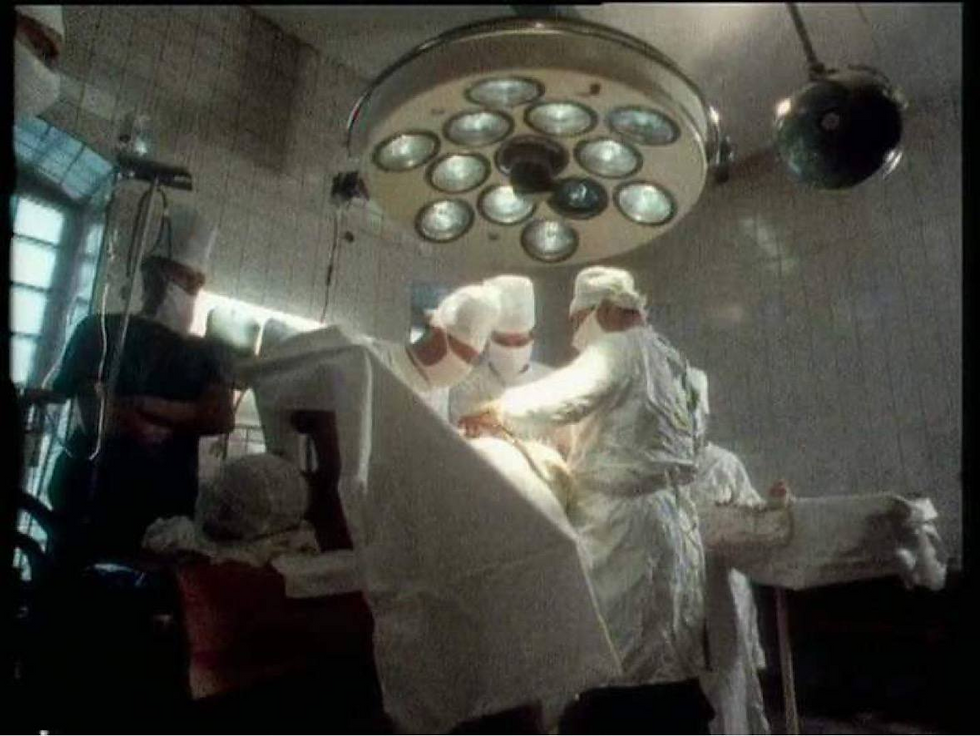
Doctors, therefore, often accompanied units into the mountains with a medic and assistant assigned to each company. A physicians assistant and a newly commissioned doctor handled initial treatment and evacuation of the wounded. A field hospital or medical post consisted of two or three doctors, a dentist, two physicians assistants, a technician, pharmacist, nurses, cook, radio operator, orderlies and driver. This would serve as a dressing station that provided immediate surgery.
The role of helicopters
The number of wounded requiring intensive treatment was much higher than expected. More rapid response and evacuation meant meant more soldiers were surviving battle wounds that previously did not. Afghanistan was a war unlike any other and the Soviet medical procedures in response to evacuation of the wounded had to change to meet the increasing number of soldiers being wounded. With timing being of the essence, ground evacuation was used increasingly with helicopter evacuation.

The seriously injured were often sent directly to the larger more equipped field hospitals or Army hospital bypassing the medical posts. As the war continued the wounded were less and less treated at medical posts and within three hours arrived at field hospitals or Army hospitals...for the most seriously injured this was crucial to survival. In 1980 this was 48% and by 1987 it had increased to just over 53%. The Mi8MB20 Bisector Medical Evacuation Helicopter was fitted out specifically for medical evacuations. Unfortunately, their carrying capacity and availability was limited leaving combat and transportation helicopters to fly the wounded to hospitals.
Soviet field medicine hospitals
Soviet Field Hospitals used two types of medical tents. The USB-56, a temporary medical tents with the capacity for 20 beds run by 40 personnel. It's heating came from two stoves with pipes leading out of the tent roof at either end. Interlocking vestibules allowed the connecting to other USB-56 tents or to the UST-56 medical tent which can then make up varying configurations as the climate and situation dictates.

The UST-56 tent has the capacity for 5 or 6 beds with 10-12 personnel. Again this tent can be attached, via vestibules or airlocks, to other standard medical tents. In almost all Soviet field hospitals throughout Afghanistan a combination of a single UST-56 tent with two USB-56 tents were used with the UST-56 tent acting as a operating room and the larger USB-56 being the pre and post operative wards.
Special surgical teams
The biggest problem was locating the wounded on the battle ground and the quality of first aid received which under such circumstances was not always ideal. Wounds faced by and treated by such combat medics and surgical teams were head wounds, stomach wounds, chest wounds, upper body wounds and leg wounds. In many cases a soldier would have multiple wounds with the most life threatening being stomach wounds and head wounds.

The Soviets formed special surgical teams to support projected military operations. The personnel came from central military hospitals and units that were not already engaged in supporting the military operation. Such teams would usually consist of three thoracic abdominal surgeons, a neurosurgeon, a traumatologist, a heart surgeon, three anesthesiologists, five surgical nurses and blood transfusion specialists.
Of these medical personnel would be formed a triage group and a specialty surgery group which would be responsible for performing thoracic abdominal surgery, neurosurgical, trauma, vascular and general surgery.
During special supported operations 90% of the wounded received first aid within 30 minutes - 80.3% were evacuated by helicopter to reinforced medical battalions.
Intensive medical support reduced time from being wounded to receiving qualified and specialized surgical care.
The statistics and the aircraft
Over 25,000 casualties between 1980-1988 were evacuated by helicopter during combat and over 152,000 sick and wounded were moved by air during some stage of their medical treatment. The air support used for these evacuations and transportations were predominantly the Mi8MB20 'Bisector' medical evacuation helicopter. Fixed wing aircraft, light medical transport, the AN26M21 'Saviour' moved the sick and wounded within Afghanistan and into the Soviet Union.

Within the Soviet Union patients were transported on a heavy military transport plane IL-76MD24 'Scalpel' or the wide bodied TU-154 passenger jet. The fixed wing propeller driven medium medical transporter IL-1822 'Orderly' moved the sick and wounded from Afghanistan to the Soviet Union. These aircraft could be rigged to carry stretchers and provide emergency in-flight medical care. During these flights 25% of patients needed intensive care. By 1987, 9% of severely wounded reached specialty hospitals within five days of being wounded and 32% within ten days. Prior to this only 1% of wounded reached hospital within five days and 5.4% within ten days.
Comments